Retake
A22) Worsening jaundice and pruritis
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Develop an understanding of the role of consulting diagnostic radiologists in the evaluation of jaundice.
- Explore the different differential diagnoses in a patient with jaundice.
- Acquire knowledge of the imaging findings and modalities used to evaluate a patient with jaundice.
History
A 30-year-old male with a prior history of ulcerative colitis presents with symptoms of gradually worsening jaundice, generalized itching, and mild fatigue over the past 6 months.
Physical Exam
Vital Signs: Blood Pressure - 134/82 mmHg, Heart Rate - 78 beats per minute, Respiratory Rate - 16 breaths per minute, Temperature - 99.8°F, Oxygen Saturation - 100%.
Skin: Yellow in appearance due to jaundice.
Eyes: PERRLA, scleral icterus present.
Abdomen: No tenderness, no distension, normal active bowel sounds, no evidence of hepatosplenomegaly.
Labs
Alkaline Phosphatase (ALP): 300 U/L (reference range: 25-100 U/L);
Gamma-glutamyl transferase (GGT): 180 U/L (reference range: 5-40 U/L);
Bilirubin: 1.5 mg/dL (reference range: 0.1-1.0 mg/dL); Conjugated fraction: 58%;
Aspartate aminotransferase (AST): 60 U/L (reference range: 10-40 U/L);
Alanine aminotransferase (ALT): 70 U/L (reference range: 7-56 U/L);
Antimitochondrial antibody: Negative.
Provisional Diagnosis
Select the Dx you believe is most appropriate
Based on the signs of cholestasis (painless jaundice, fatigue, and elevated ALP, GGT, and conjugated bilirubin levels) in a young male with a history of ulcerative colitis, the most likely diagnosis is primary sclerosing cholangitis. This condition is commonly associated with chronic inflammatory bowel disease, with around 90% of patients with primary sclerosing cholangitis having ulcerative colitis.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient’s condition is not immediately life threatening.
First Imaging Study
What is the first imaging study you will order?
ERCP or MRCP is the preferred imaging study for evaluating the biliary tree in this patient.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
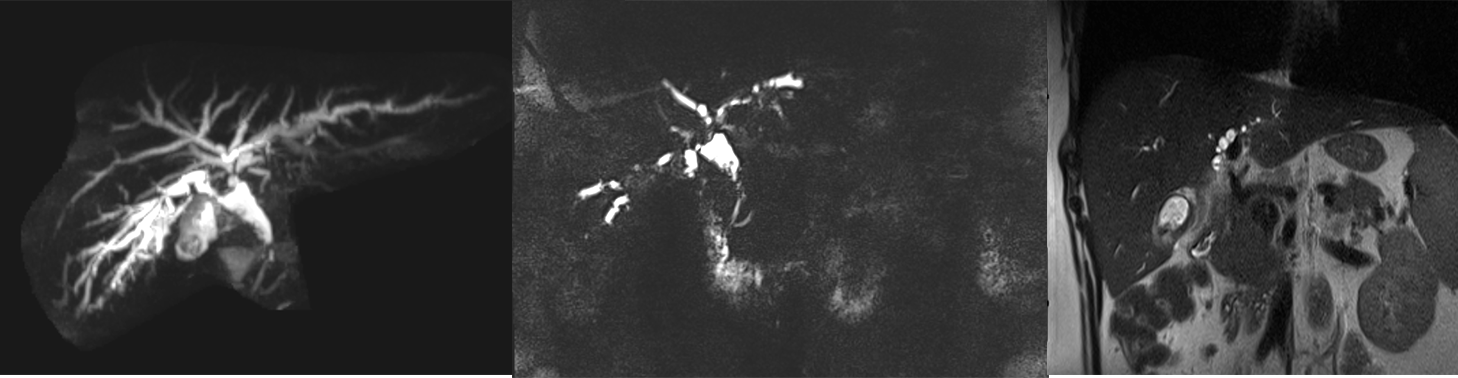
MRCP with and without contrast
Which regions show evidence of inflammatory changes?
There is diffuse dilatation, beading, and stricturing in both the intrahepatic and extrahepatic bile ducts.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
None. The MRCP was sufficient to make the diagnosis.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
Primary sclerosing cholangitis is a chronic and progressive inflammatory condition that affects both the intrahepatic and extrahepatic bile ducts. Multifocal beading is a classic feature of this disease. It is most common in middle-aged men and is strongly associated with inflammatory bowel disease, particularly ulcerative colitis. Primary biliary cholangitis, on the other hand, is an autoimmune disease that affects only the intrahepatic bile ducts and is more common in women. Negative antimitochondrial antibody can help exclude this diagnosis. Secondary sclerosing cholangitis is caused by an underlying condition such as chronic biliary obstruction or trauma/injury to the biliary tree.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient’s condition is not immediately life-threatening.
Assessment and Plan
Please provide your assessment and plan for this patient
A 30-year-old male with ulcerative colitis has been experiencing gradual onset jaundice and mild fatigue for 1.5 weeks. Lab tests showed elevated ALP, GGT, and conjugated bilirubin, while MRCP with contrast indicated multifocal beading and stricture in both intrahepatic and extrahepatic bile ducts. The patient's condition is suspected to be primary sclerosing cholangitis (PSC), and he should be referred to a hepatologist. Symptomatic relief and slowed disease progression can be achieved through ursodeoxycholic acid, while topical antihistamines or emollients can be used to manage pruritis. The patient should be reminded of the importance of taking fat-soluble vitamin supplements (A, D, E, K) due to malabsorption related to cholestasis. Additionally, the patient should be informed of the possible complications of PSC, such as cirrhosis, cholangiocarcinoma, and the potential need for a liver transplant.
Lessons Learned:
- Primary sclerosing cholangitis is a chronic and progressive inflammatory condition that affects both the intrahepatic and extrahepatic bile ducts. Multifocal beading is a classic feature.
- Primary sclerosing cholangitis is most common in middle-aged men and is strongly associated with inflammatory bowel disease, particularly ulcerative colitis.
- Primary biliary cholangitis is an autoimmune disease that affects only the intrahepatic bile ducts and is more common in women. Negative antimitochondrial antibody titers can help exclude this diagnosis.
- Secondary sclerosing cholangitis is caused by an underlying condition such as chronic biliary obstruction or trauma/injury to the biliary tree.
- Median survival without liver transplantation after diagnosis is 10 to 21 years, and survival is significantly worse for patients who are symptomatic at the time of diagnosis.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}